- Hits: 5589





Metastasis. In metastasis, cancer cells break away from where they first formed (primary cancer), travel through the blood or lymph system, and form new tumors (metastatic tumors) in other parts of the body. The metastatic tumor is the same type of cancer as the primary tumor.
We're for all- ALL are for us for the greater interest of Humanism-Truth-Facts-Friendship-A'1 Unity-PEACE-Participation-No"War-Poverty-Cruelty- Discrimination", FREE Democracy with STATE based Strong Sovereignty+ including Physico-Mental Sound Healths++ with Spirituality, enrichment through ''TOTAL HEALTH SOLUTION'' to reach a Well-furnished "GOAL of Truth" fixed for all in real sense of Universal Rules & Regulations by Omniscience+++++ ;
From wikipedia & other reliable sources (Poets, Writers, Thinkers, Researchers, Free Lancers, Philosophers, Theologists, Scientists, Orators, Sociologists and Photographers +Artists-Musicians & UN etc.) we can learn as follows :
It's Completely a Step by Step "Global UN-Members State" based Comparative Health Program Explanation Studies in favor of "Total Health Solution Crisis Mitigation" including Breast Cancers Free World" ASSURING "No Deaths of Mothers, Women, Youths, Teenagers, Adolescents, Children, Babies & Next Generation etc. from NOW":- by the Treatment of ongoing "Health Restoring Systems +Managements" available Globally everywhere for 800 Crores Human-beings, having No fruitful Curative Means of Accuracy to recover PATIENTS properly+++; including Natural Restoration based on insufficient "Knowledge & Experiences about 'Environmental Cycling Procedures++' which drive "Global+++ Nature" Properly & Permanently, within "Universal-friendly Limit" according to "Universal Mysteries" have forever beyound our Limitation Carry out, we're possible accordingly for our very existences in the world.
Our "First-Form" is as follows for your Physical-Mental special-Emergency Medical Services always (Day & Night Everwhere to Everone Globally):
Metastatic breast cancer, also referred to as metastases, advanced breast cancer, secondary tumors, secondaries or stage IV breast cancer, is a stage of breast cancer where the breast cancer cells have spread to distant sites beyond the axillary lymph nodes. Wikipedia
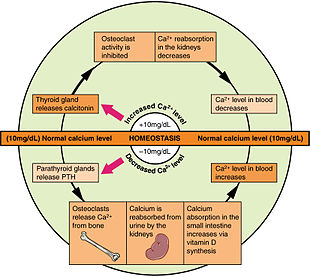
In biology, homeostasis is the state of steady internal physical and chemical conditions maintained by living systems. This is the condition of optimal functioning for the organism and includes many variables, such as body temperature and fluid balance, being kept within certain pre-set limits. Wikipedia



![]()

Human iron metabolism is the set of chemical reactions that maintain human homeostasis of iron at the systemic and cellular level. Iron is both necessary to the body and potentially toxic. Controlling iron levels in the body is a critically important part of many aspects of human health and
Copper is an essential trace element that is vital to the health of all living things (plants, animals and microorganisms). In humans, copper is essential to the proper functioning of organs and metabolic processes. Also, in humans, copper helps maintain the nervous system, immune system, brain development, and activates genes, as well as assisting in the production of connective tissues, blood vessels, and energy.[1] The human body has complex homeostatic mechanisms which attempt to ensure a constant supply of available copper, while eliminating excess copper whenever this occurs. However, like all essential elements and nutrients, too much or too little nutritional ingestion of copper can result in a corresponding condition of copper excess or deficiency in the body, each of which has its own unique set of adverse health effects.
The respiratory center is located in the medulla oblongata and pons, in the brainstem. The respiratory center is made up of three major respiratory groups of neurons, two in the medulla and one in the pons. In the medulla they are the dorsal respiratory group, and the ventral respiratory group. In the pons, the pontin
The renin–angiotensin system (RAS), or renin–angiotensin–aldosterone system (RAAS), is a hormone system that regulates blood pressure, fluid and electrolyte balance, and systemic vascular resistance.
The aorta is the main and largest artery in the human body, originating from the left ventricle of the heart, branching upwards immediately after, and extending down to the abdomen, where it splits at the aortic bifurcation into two smaller arteries. The aorta distributes oxygenated blood to all parts of the body through the
Calcium metabolism is the movement and regulation of calcium ions (Ca2+) in (via the gut) and out (via the gut and kidneys) of the body, and between body compartments: the blood plasma, the extracellular and intracellular fluids, and bone. Bone acts as a calcium storage center for





COMMENTS FROM Dr. P. C. Majumder (- Author. Writer, Humanist, Physician (Physico-Mental & Spiritual) and Cosmopolitan Researcher in favor of ALL-CREATION Universally RESIDE++++ in positive ways for universal UNITY & LOVE++++) as follows:
1. Congratulation to "ALL MEMBER STATES IN UN" for their Most Positivity, with proper Participation & Cordiality to enhance "Health Services to All reside in the World" unitedly like COVID-'19 Pandemics where every Health initiative performed to solve primarily, how "COVID'19 Fatality OVER step by step, and saving Life & resist Unexpected Deaths" without 'CURATIVE HEALTH SOLUTION'.
2. Now, WE NEED a Most Urgent/ Step by Step initiative to provide proper & Ideal A'1 CURATIVE TRIPLE HEALTH SOLUTION as early as possible instead of present ongoing "Palliative, Protective, Preventive, Short acting Medicines-Prescription including Life-threatening side effects based Conditional BRUTAL SURGERIES" done around globally.
Contd.
We're for all- ALL are for us for the greater interest of Humanism-Truth-Facts-Friendship-Unity-PEACE-Participation-"War, Poverty, Cruelty, Discrimination" FREE Democracy with STATE based Strong Sovereignty+ to reach a Well-defined GOAL of Truth from which All shall have over all ++++Social Human Standards ;
We're indebted to WIKIPEDIA +UNITED NATIONS & WHO etc. for a short while and as 'Guardian QUOTATION' from Global WISER ONE. And have quoted many images, article's, writings etc. by great & humanist writers+++ from global thinkers, Well-wishers, Wiseman, Humanists and Others Living-Nonlivings in favor of HUMANISM to share more answers of Researchers-readers+++++.... ASKINGS+++++.
To reach the 'GOAL of FULFILNESS' unitedly to alive in the "DESTINATION of TRUTH-FACTS-CHARMEST AMICABLITY" of Natural Joyful POSSIBILITIES+++
BREAST CANCERs, Cancers, Tuberculosis, All sorts of Fevers like Malaria, Typhoid, Dengue, other infections, Asthma, Hereditary Asthma, TUMORS, Arsenic Poisoning +Other Chemical Poisoning, All sorts of Flu-Corona(SARS, MARS, COVID-19 like Complexities), Heart-Lung diseases, Neurological-Hormonal-Immunal-Infectious diseases with related Complexities including ALL SORTS OF PHYSICO-MENTAL DISEASES & DISORDERS are Possible to CURE properly-easily-scientifically-accurately (100%+) by our "Ideal Curative Medical Services" only with "+++++Balanced Mutual Confirmation". We never use "Palliative, Protective, Preventive, Short acting Medicines and Major Life Threatening Surgeries which have life-long Fatality, Complexity +Unexpected Death Consequences".
Medicines-Foods control-proper close nursing-medicinal massage-Medicinal Yogas- Meditation, Physiotherapy special etc. without side effects & Repeatation as per contract through user-friendly approved ways of CURE++++. please fill our form as above & Submit to evaluate for a Most Urgent Ideal A'1 Curative Triple Health Solution Globe-widely.
After confirming contract-letter between you+++. We serve you properly with "No Side Effects based Chemotherapy-radiation therapy -SURGICAL Complexities (Physical-Mental) to a Most Urgent Ideal A'1 CURATIVE-Effects+++ up to our Limits to recover your both-health from illness+.

- Hits: 1245

![]()
We're for all- ALL are for us for the greater interest of Humanism-Truth-Facts-Friendship-A'1 Unity-PEACE-Participation-No"War-Poverty-Cruelty- Discrimination", FREE Democracy with STATE based Strong Sovereignty+ including Physico-Mental Sound Healths++ with Spirituality, enrichment through ''TOTAL HEALTH SOLUTION'' to reach a Well-furnished "GOAL of Truth" fixed for all in real sense of Universal Rules & Regulations by Omniscience+++++ ;
From wikipedia & other reliable sources (Poets, Writers, Thinkers, Researchers, Free Lancers, Philosophers, Theologists, Scientists, Orators, Sociologists and Photographers +Artists-Musicians & UN etc.) we can learn as follows :
It's Completely a Step by Step "Global UN-Members State" based Comparative Health Program Explanation Studies in favor of "Total Health Solution Crisis Mitigation" including Breast Cancers Free World" ASSURING "No Deaths of Mothers, Women, Youths, Teenagers, Adolescents, Children, Babies & Next Generation etc. from NOW" by the Treatment of ongoing "Health Restoring Systems +Managements available Globally among, for 800 Crores Human-beings including Natural Restoration Properly & Permanently according to our Limitation Carry out.
The right to health is an inclusive right, extending not only to timely and appropriate health care, but also to the underlying determinants of health, such as access to safe and potable water and adequate sanitation, healthy occupational and environmental conditions, and access to health-related education and ...
Health is a fundamental right of every human being. Health as a human right is recognized in the WHO Constitution (1948), the Universal Declaration of Human Rights (1948) and many international and regional human rights treaties. All WHO Member States have ratified at least one treaty that recognizes the right to the highest attainable standard of physical and mental health.
This means that countries have legal obligations, while acknowledging that time and resources are required to fully achieve them. Some immediate obligations for countries include the guarantees of non-discrimination and equal treatment in health. The right to health includes entitlements, such as the right to control one’s health, informed consent, bodily integrity, and participation in health-related decision-making. It also includes freedoms, like freedom from torture, ill-treatment and harmful practices.
The right to health is closely related to and dependent on the realization of other human rights, including the rights to life, food, housing, work, education, privacy, access to information, freedom from torture and the freedoms of association, assembly and movement. It includes both nondiscriminatory access to quality, timely and appropriate health services and systems and to the underlying determinants of health.
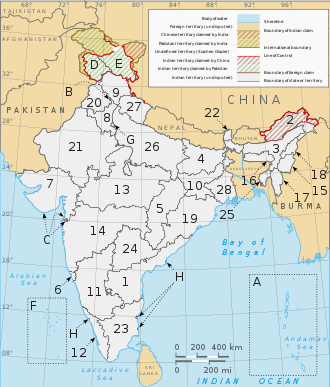
Global Health- India with Basic Health Crisis of most population through PPP(Palliative-Preventive-Protective} Management by Short acting Side Effects based availability instead of Curative A'1 Ideal Triple Health Solution.

![]()








![]()
![]()



![]()


![]()
According to a Food and Agriculture Organization report in 2015, 15% of the population is undernourished.[354][355] The Midday Meal Scheme attempts to lower these rates.[356]
The Indian state Tamil Nadu was a pioneer in introducing midday meal programmes in India to increase the number of children enrolling in school; K. Kamaraj, the Chief Minister of Tamil Nadu at the time, introduced it first in Chennai and later extended it to all districts of Tamil Nadu.[12] During 1982, 1 July onwards, the Chief Minister of Tamil Nadu, M. G. Ramachandran upgraded the existing midday meal scheme in the state to 'Nutritious noon-meal scheme'[13] keeping in mind that around 68 lakh children were malnourished.[14] Gujarat was the second state to introduce an MDM scheme in 1984, but it was later discontinued.[15]
A midday meal scheme was introduced in Kerala in 1984, and was gradually expanded to include more schools and grades.[16] By 1990–91, twelve states were funding the scheme to all or most of the students in their area: Goa, Gujarat, Kerala, Madhya Pradesh, Maharashtra, Meghalaya, Mizoram, Nagaland, Sikkim, Tamil Nadu, Tripura and Uttar Pradesh. Karnataka, Odisha and West Bengal received international aid to help with the implementation of the programme, while in AP and Rajasthan the programme was completely funded by foreign aid.[17]
In Karnataka, the Children's LoveCastles Trust started providing midday meals in 1997. A total of eight schools were adopted and a food bank programme and an Angganwasi milk Programme were started. The food-bank programme was replaced by the State Government midday meal scheme.[18]



Supreme court order[edit]
In April 2001, the People's Union for Civil Liberties (PUCL) initiated the Public Interest Litigation (Civil) No. 196/2001, People's Union for Civil Liberties v. Union of India & Others[21] – popularly known as the "right to food" case. The PUCL argued that article 21 – "right to life" of the Indian constitution when read together with articles 39(a) and 47, makes the right to food a derived fundamental right which is enforceable by virtue of the constitutional remedy provided under article 32 of the constitution. The PUCL argued that excess food stocks with the Food Corporation of India should be fed to hungry citizens. This included providing midday meals in primary schools. The scheme came into force with the supreme court order dated 28 November 2001,[22] which requires all government and government-assisted primary schools to provide cooked midday meals.[23]
President Pranab Mukherjee launching mid-day meal scheme at a Central Government-run school
Interim orders[edit]
The Supreme Court occasionally issues interim orders regarding midday meals.[24] Some examples are:[23]
| Order regarding | Exact text | Order dated |
|---|---|---|
| Basic entitlement | "Every child in every place and Government assisted Primary Schools with a prepared midday meal with a minimum content of 300 calories and 8–12 grams of protein each day of school for a minimum of 200 days" | 28 November 2001[25] |
| Charges on conversion cost | "The conversion costs for a cooked meal, under no circumstances, shall be recovered from the children or their parents" | 20 April 2004[26] |
| Central assistance | "The Central Government... shall also allocate funds to meet with the conversion costs of food-grains into cooked midday meals" | 20 April 2004[26] |
| Kitchen sheds | "The Central Government shall make provisions for construction of kitchen sheds" | 20 April 2004[26] |
| Priority to Dalit cooks | "In appointment of cooks and helpers, preference shall be given to Dalits, Scheduled Castes and Scheduled Tribes" | 20 April 2004[26] |
| Quality safeguards | "Attempts shall be made for better infrastructure, improved facilities (safe drinking water etc.), closer monitoring (regular inspection etc.) and other quality safeguards as also the improvement of the contents of the meal so as to provide nutritious meal to the children of the primary schools" | 20 April 2004[26] |
| Drought areas | "In drought affected areas, midday meals shall be supplied even during summer vacations" | 20 April 2004[26] |
Entitlements[edit]
The nutritional guidelines for the minimum amount of food and calorie content per child per day are:[3]
| Item | Primary (class one to five) | Upper primary (class six to eight) |
|---|---|---|
| Calories | 450 | 700 |
| Protein (in grams) | 12 | 20 |
| Rice / wheat (in grams) | 100 | 150 |
| Dal (in grams) | 20 | 30 |
| Vegetables (in grams) | 50 | 75 |
| Oil and fat (in grams) | 5 | 7.5 |
In the case of micronutrients (vitamin A, iron, and folate) tablets and de-worming medicines, the student is entitled to receive the amount provided for in the school health programme of the National Rural Health Mission.[27]
Finances[edit]
The central and state governments share the cost of the Midday Meal Scheme, with the centre providing 60 percent and the states 40 percent.[28] The central government provides grains and financing for other food. Costs for facilities, transportation, and labour is shared by the federal and state governments.[29] The participating states/territories contribute different amounts of money, depending on whether they are Himalayan states, Northeastern Region (NER) states, union territories without legislature, or the residual (Non-NER states and union territories with legislature).[23][30] The share contributed by states is often larger than what is stipulated. While the eleventh five-year plan allocated ₹384.9 billion (equivalent to ₹450 billion or US$5.4 billion in 2023) for the scheme, the twelfth five-year plan has allocated ₹901.55 billion (US$11 billion), a 134 percent rise.[31] The public expenditure for the Mid Day Meal Programme has gone up from ₹73.24 billion (US$880 million) in 2007–08 to ₹132.15 billion (US$1.6 billion) in 2013–14.[32] In 2020–21, the Midday Meal Scheme budget comprised 11% of the total budget for the Ministry of Education.[30] The per day cooking cost per child at the primary level has been fixed to ₹4.13 (4.9¢ US) while at the upper primary level is ₹6.18 (7.4¢ US).[33]
Tithi Bhojan is a concept designed to ensure greater public participation under the Midday Meal Programme, that started out in the state of Gujarat. In order to generate greater community participation, local members were encouraged to celebrate social events like birth of a child and homewarming by donating to the midday meals served in the local schools. It is voluntarily served by the community/family among school children in several forms such as sweets and savoury snacks, along with regular MDM, full meals, supplementary nutritive items like sprouted beans, and contributions in kind such as cookware, utensils, dinner sets or glasses for drinking water. The concept has been adopted by 10 other states, some with local nomenclatures like "Sampriti Bhojan" in Assam, "Dham" in Himachal Pradesh, "Sneh Bhojan" in Maharashtra, "Shalegagi Naavu Neevu" in Karnataka, "Anna Dhanam" in Puducherry, "Priti Bhoj" in Punjab and "Utsav Bhoj" in Rajasthan. In the North Indian states of Uttarakhand, Haryana and the Union territory of Chandigarh, the scheme retains its original name of Tithi Bhojan.[41]
![]()






![]()



![]()
![]()



COMMENTS FROM Dr. P. C. Majumder (- Author. Writer, Humanist, Physician (Physico-Mental & Spiritual) and Cosmopolitan Researcher in favor of ALL-CREATION Universally RESIDE++++ in positive ways for universal UNITY & LOVE++++) as follows:
1. Congratulation to "ALL MEMBER STATES IN UN" for their Most Positivity, with proper Participation & Cordiality to enhance "Health Services to All reside in the World" unitedly like COVID-'19 Pandemics where every Health initiative performed to solve primarily, how "COVID'19 Fatality OVER step by step, and saving Life & resist Unexpected Deaths" without 'CURATIVE HEALTH SOLUTION'.
2. Now, WE NEED a Most Urgent/ Step by Step initiative to provide proper & Ideal A'1 CURATIVE TRIPLE HEALTH SOLUTION as early as possible instead of present ongoing "Palliative, Protective, Preventive, Short acting Medicines-Prescription including Life-threatening side effects based Conditional BRUTAL SURGERIES" done around globally.
Contd.
We're for all- ALL are for us for the greater interest of Humanism-Truth-Facts-Friendship-Unity-PEACE-Participation-"War, Poverty, Cruelty, Discrimination" FREE Democracy with STATE based Strong Sovereignty+ to reach a Well-defined GOAL of Truth from which All shall have over all ++++Social Human Standards ;
We're indebted to WIKIPEDIA +UNITED NATIONS & WHO etc. for a short while and as 'Guardian QUOTATION' from Global WISER ONE. And have quoted many images, article's, writings etc. by great & humanist writers+++ from global thinkers, Well-wishers, Wiseman, Humanists and Others Living-Nonlivings in favor of HUMANISM to share more answers of Researchers-readers+++++.... ASKINGS+++++.
To reach the 'GOAL of FULFILNESS' unitedly to alive in the "DESTINATION of TRUTH-FACTS-CHARMEST AMICABLITY" of Natural Joyful POSSIBILITIES+++
BREAST CANCERs, Cancers, Tuberculosis, All sorts of Fevers like Malaria, Typhoid, Dengue, other infections, Asthma, Hereditary Asthma, TUMORS, Arsenic Poisoning +Other Chemical Poisoning, All sorts of Flu-Corona(SARS, MARS, COVID-19 like Complexities), Heart-Lung diseases, Neurological-Hormonal-Immunal-Infectious diseases with related Complexities including ALL SORTS OF PHYSICO-MENTAL DISEASES & DISORDERS are Possible to CURE properly-easily-scientifically-accurately (100%+) by our "Ideal Curative Medical Services" only with "+++++Balanced Mutual Confirmation". We never use "Palliative, Protective, Preventive, Short acting Medicines and Major Life Threatening Surgeries which have life-long Fatality, Complexity +Unexpected Death Consequences".
Medicines-Foods control-proper close nursing-medicinal massage-Medicinal Yogas- Meditation, Physiotherapy special etc. without side effects & Repeatation as per contract through user-friendly approved ways of CURE++++. please fill our form as above & Submit to evaluate for a Most Urgent Ideal A'1 Curative Triple Health Solution Globe-widely.
After confirming contract-letter between you+++. We serve you properly with "No Side Effects based Chemotherapy-radiation therapy -SURGICAL Complexities (Physical-Mental) to a Most Urgent Ideal A'1 CURATIVE-Effects+++ up to our Limits to recover your both-health from illness+.
- Hits: 516
We're for all- ALL are for us for the greater interest of Humanism-Truth-Facts-Friendship-Unity-PEACE-Participation-"War, Poverty, Cruelty, Discrimination" FREE Democracy with STATE based Strong Sovereignty+ to reach a Well-defined GOAL of Truth from which All shall have over all ++++Social Human Standards ;
We're indebted to WIKIPEDIA +UNITED NATIONS & WHO etc. for a short while and as 'Guardian QUOTATION' from Global WISER ONE. And have quoted many images, article's, writings etc. by great & humanist writers+++ from global thinkers, Well-wishers, Wiseman, Humanists and Others Living-Nonlivings in favor of HUMANISM to share more answers of Researchers-readers+++++.... ASKINGS+++++.
To reach the 'GOAL of FULFILNESS' unitedly to alive in the "DESTINATION of TRUTH-FACTS-CHARMEST AMICABLITY" of Natural Joyful POSSIBILITIES+++
BREAST CANCERs, Cancers, Tuberculosis, All sorts of Fevers like Malaria, Typhoid, Dengue, other infections, Asthma, Hereditary Asthma, TUMORS, Arsenic Poisoning +Other Chemical Poisoning, All sorts of Flu-Corona(SARS, MARS, COVID-19 like Complexities), Heart-Lung diseases, Neurological-Hormonal-Immunal-Infectious diseases with related Complexities including ALL SORTS OF PHYSICO-MENTAL DISEASES & DISORDERS are Possible to CURE properly-easily-scientifically-accurately (100%+) by our "Ideal Curative Medical Services" only with "+++++Balanced Mutual Confirmation". We never use "Palliative, Protective, Preventive, Short acting Medicines and Major Life Threatening Surgeries which have life-long Fatality, Complexity +Unexpected Death Consequences".
Medicines-Foods control-proper close nursing-medicinal massage-Medicinal Yogas- Meditation, Physiotherapy special etc. without side effects & Repeatation as per contract through user-friendly approved ways of CURE++++. please fill our form as above & Submit to evaluate for a Most Urgent Ideal A'1 Curative Triple Health Solution Globe-widely.
If there is any mistakes, plz inform me at "First prescription"- I'll generally correct the same assuring mistakes with "No Doughts'.
Pain is a signal in your nervous system that something may be wrong. It is an unpleasant feeling, such as a prick, tingle, sting, burn, or ache. Pain may be sharp or dull. It may come and go, or it may be constant.
Pain is a distressing feeling often caused by intense or damaging stimuli. The International Association for the Study of Pain defines pain as "an unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage." Wikipedia
Medication: Analgesic
Symptoms: Unpleasant sensory and emotional sensations
Duration: Typically depends on the cause




Pain is the most common reason for physician consultation in most developed countries.[4][5] It is a major symptom in many medical conditions, and can interfere with a person's quality of life and general functioning.[6] People in pain experience impaired concentration, working memory, mental flexibility, problem solving and information processing speed, and are more likely to experience irritability, depression, and anxiety.
Simple pain medications are useful in 20% to 70% of cases.[7] Psychological factors such as social support, cognitive behavioral therapy, excitement, or distraction can affect pain's intensity or unpleasantness.[8][9]
Rheumatic symptoms (or rheumatism) are distinguished by the following seven characteristics: (1) pain or discomfort, usually perceived in the vicinity of one or more joints (including the spine); (2) pain on motion of the affected area(s); (3) soreness (to the touch) of the affected region(s); (4) stiffness of the ...
"Pain Management Specialists - Pain Management Physicians" say as follows:
They engage for relieving palliatively following Pains of sufferers with good managements ++:
From Head to Toe - We Specialize in the Diagnosis & Treatment of Chronic Pain. Board Certified Pain Physicians. Veterans Choice Approved. Interventional Treatments. We Treat All Pain. Since 1999. Convenient Locations.
After confirming contract-letter between you+++. We serve you properly with "No Side Effects based Chemotherapy-radiation therapy -SURGICAL Complexities (Physical-Mental) to a Most Urgent Ideal A'1 CURATIVE-Effects+++ up to our Limits to recover your both-health from illness+.
COMMENTS FROM Dr. P. C. Majumder (- Author. Writer, Humanist, Physician (Physico-Mental & Spiritual) and Cosmopolitan Researcher in favor of ALL-CREATION Universally RESIDE++++ in positive ways for universal UNITY & LOVE++++) as follows:
1. Congratulation to "ALL MEMBER STATES IN UN" for their Most Positivity, with proper Participation & Cordiality to enhance "Health Services to All reside in the World" unitedly like COVID-'19 Pandemics where every Health initiative performed to solve primarily, how "COVID'19 Fatality OVER step by step, and saving Life & resist Unexpected Deaths" without 'CURATIVE HEALTH SOLUTION'.
2. Now, WE NEED a Most Urgent/ Step by Step initiative to provide proper & Ideal A'1 CURATIVE TRIPLE HEALTH SOLUTION as early as possible instead of present ongoing "Palliative, Protective, Preventive, Short acting Medicines-Prescription including Life-threatening side effects based Conditional BRUTAL SURGERIES" done around globally.
- Hits: 424
Hypertension, Heart Diseases, Diabetic, Liver-Kidney Diseases, & Stroke Complexity
We're for all- ALL are for us for the greater interest of Humanism-Truth-Facts-Friendship-Unity-Participation including Physico-Mental Sound Health with Spirituality, enrichment through ''TOTAL HEALTH SOLUTION'' to a Well-furnished GOALofTruth alloted for all in real sense ;
From wikipedia & other reliable sources (Poets, Writers, Thinkers, Researchers, Free Lancers, Philosophers, Theologists, Scientists, Orators, Sociologists and Photographers +Artists-Musicians & UN etc.) we can learn as follows :
Hypertension (high blood pressure) is when the pressure in your blood vessels is too high (140/90 mmHg or higher). It is common but can be serious if not treated. People with high blood pressure may not feel symptoms.
Hypertension, also known as high blood pressure, is a long-term medical condition in which the blood pressure in the arteries is persistently elevated.[11] High blood pressure usually does not cause symptoms itself.[1] It is, however, a major risk factor for stroke, coronary artery disease, heart failure, atrial fibrillation, peripheral arterial disease, vision loss, chronic kidney disease, and dementia.[2][3][4][12] Hypertension is a major cause of premature death worldwide.[13]
High blood pressure is classified as primary (essential) hypertension or secondary hypertension.[5] About 90–95% of cases are primary, defined as high blood pressure due to nonspecific lifestyle and genetic factors.[5] Lifestyle factors that increase the risk include excess salt in the diet, excess body weight, smoking, physical inactivity and alcohol use.[1][5] The remaining 5–10% of cases are categorized as secondary hypertension, defined as high blood pressure due to a clearly identifiable cause, such as chronic kidney disease, narrowing of the kidney arteries, an endocrine disorder, or the use of birth control pills.[5]
Blood pressure is classified by two measurements, the systolic (first number) and diastolic (second number) pressures.[1] For most adults, normal blood pressure at rest is within the range of 100–140 millimeters mercury (mmHg) systolic and 60–90 mmHg diastolic.[6][7] For most adults, high blood pressure is present if the resting blood pressure is persistently at or above 130/80 or 140/90 mmHg.[5][6][7] Different numbers apply to children.[14] Ambulatory blood pressure monitoring over a 24-hour period appears more accurate than office-based blood pressure measurement.[5][11]
Lifestyle changes and medications can lower blood pressure and decrease the risk of health complications.[8] Lifestyle changes include weight loss, physical exercise, decreased salt intake, reducing alcohol intake, and a healthy diet.[5] If lifestyle changes are not sufficient, blood pressure medications are used.[8] Up to three medications taken concurrently can control blood pressure in 90% of people.[5] The treatment of moderately high arterial blood pressure (defined as >160/100 mmHg) with medications is associated with an improved life expectancy.[15] The effect of treatment of blood pressure between 130/80 mmHg and 160/100 mmHg is less clear, with some reviews finding benefit[6][16][17] and others finding unclear benefit.[18][19][20] High blood pressure affects 33% of the population globally.[9] About half of all people with high blood pressure do not know that they have it.[9] In 2019, high blood pressure was believed to have been a factor in 19% of all deaths (10.4 million globally).[9]






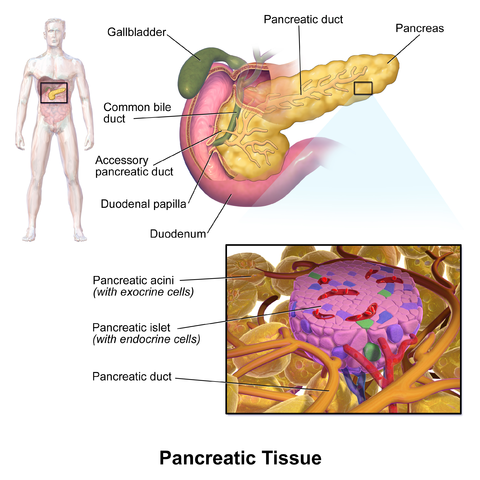
Diabetes is a chronic disease that occurs either when the pancreas does not produce enough insulin or when the body cannot effectively use the insulin it produces. Insulin is a hormone that regulates blood glucose.



Coronary artery disease (CAD), also called coronary heart disease (CHD), ischemic heart disease (IHD),[13] myocardial ischemia,[14] or simply heart disease, involves the reduction of blood flow to the cardiac muscle due to build-up of atherosclerotic plaque in the arteries of the heart.[5][6][15] It is the most common of the cardiovascular diseases.[16] Types include stable angina, unstable angina, and myocardial infarction.[17]
Most read

Metastasis. In metastasis, cancer cells break away from where they first formed (primary ...

We're for all- ALL are for us for the greater interest of Humanism-Truth-Facts-Friendship-A'1 ...

We're for all- ALL are for us for the greater interest of Humanism-Truth-Facts-Friendship-A'1 ...


রক্তরোগ (থ্যালাসেমিয়া, প্লাটিলেট সমস্যা/প্রাণঘাতি ইনফেক্শন, ব্লাড-ক্যান্সার ইত্যাদি) ও ...

Hypertension, Heart Diseases, Diabetic, Liver-Kidney Diseases, & Stroke Complexity
We're for ...

Patient Form for Appointment, Registration, Patient Case-Report, Primary Prescription, ...

The Nobel Prize in Physiology & Medicines 2023
The following "Scientific ...

Patient, Physician & Medical Services are most close-related Components of our
Life ...


Now-a-days Breast Cancers & Fatal Female Diseases are epidemic like Basic Human Health Crisis ...

We quote here the study of wikipedia for comparative reference
Metastatic breast cancer, also ...

HEALTH-CONSCIOUSNESS
PHYSICO-MENTAL COMMUNITY HEALTH CLINIC
A SISTER CONCERN OF “HEALTH ...

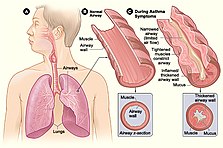
Asthma, COVID-19 and Cancers - হাঁপানী/শ্বাসকষ্ট/করোনা/ফ্ল-Ads
ASthma/Bronchitis/COVID'19 - হাঁপানী/শ্বাসকষ্ট/করোনা/ফ্ল
Asthma is a major noncommunicable disease (NCD), affecting both children and adults, and is the most common chronic disease among children. Inflammation and narrowing of the small airways in the lungs cause asthma symptoms, which can be any combination of cough, wheeze, shortness of breath and chest tightness.